In April 2020, COVAX was set up to accelerate the development, manufacture, and globally fair allocation of COVID-19 vaccines. COVAX set an objective of procuring two billion doses of safe, effective vaccine by the end of 2021, and used advanced purchasing commitments as a specific mechanism to provide vaccines to the poorest low- and middle-income countries (AMC92).
When COVAX was established, there was scientific uncertainty around whether an efficacious vaccine against a coronavirus could be developed at all. And on the manufacturing side, prior to COVID-19, estimated annual global vaccine demand was around 3.5 billion doses (excluding an estimated 1.5 billion doses for seasonal influenza), and the feasibility of a scale-up without time to construct new facilities was also unknown.
Despite these uncertainties, as of 25 October 2021, 14 safe and efficacious vaccines were developed and over 6.5 billion doses have been procured or donated via the COVAX Facility within a year of the first vaccine licensure. Over 7.8 billion doses have been delivered globally; just over 400 million of these doses have been delivered by COVAX to 144 countries/territories. The delivery of doses to low- and middle-income countries has lagged disappointingly, and many countries remain dramatically less vaccinated than high-income countries.
Figure 1. Timeline of key events and milestones
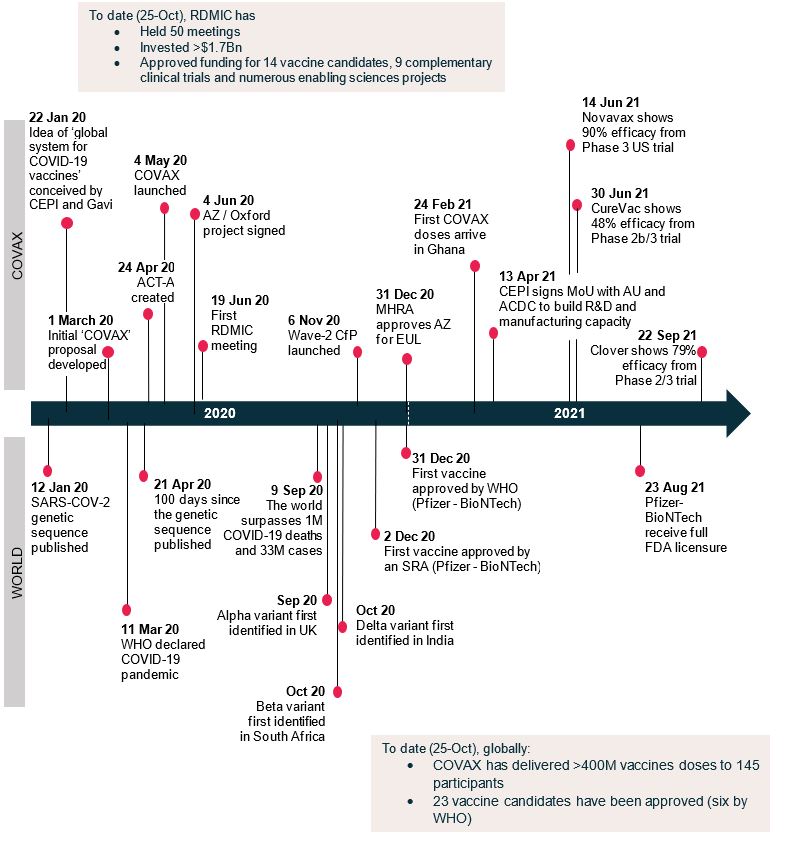
Source: Summary of findings of COVAX R&D and manufacturing investment review (Appendix)
We conducted a joint review of the portfolio management activities of the committee overseeing COVAX R&D and manufacturing investments, known as RDMIC (R&D and Manufacturing Investment Committee). COVAX was set up with 4 workstreams, one of which is Development and Manufacturing, with the RDMIC operating as an expert advisory group, making recommendations to the CEPI Board for investment. Our aim was to assess learnings from investments to date and suggest ways to strengthen future global health security preparedness and prevent the inequities observed in the COVID-19 response from repeating (see Appendix for the detailed findings of the review).
Key findings
-
RDMIC was successful in developing a highly diversified portfolio of vaccine candidates despite uncertainty on vaccine technologies and mechanisms of action as well as capabilities of different companies. Fourteen vaccine candidates were financed, and multiple firms developed and manufactured enormous quantities of vaccine in a historically short period.
-
RDMIC was able to identify and mitigate some key manufacturing risks on an ongoing basis: early on, challenges were identified in technology transfers from originators to partnering manufacturers, and a dedicated team was established to work directly with firms to manage these risks. RDMIC also secured and centrally managed supplies of adjuvant and materials (e.g., medical glass) to enable continued progress on manufacturing.
-
However, more could have been done to mitigate regulatory and manufacturing risks through closer direct engagement with developers and manufacturers, particularly those with less experience. R&D push money provided by CEPI did not generate sufficient insight into and leverage with firms, nor was it sufficient to reserve doses for advance purchase agreements early and before the conclusion of phase III trials. More broadly across COVAX, delays in initiating advanced purchase agreements meant that they had to compete with bilateral purchasers on the market. In addition, political risks due to nationalism (for example, export restrictions on doses produced by manufacturers in India—resulting in significant delays to delivery of doses to low- and middle-income countries) were underappreciated.
-
Funding available to COVAX’s development and manufacturing workstream was entirely inadequate given the scale of the challenge. Whereas Operation Warp Speed invested $12.4 billion to develop and manufacture vaccines for the US, equating to $38 per capita, COVAX had $1.7 billion available to cover the global population, equating to around 22 cents per capita. The market power was simply not there to respond early and effectively to a global pandemic. As a result of restricted funding, investment decisions and risk management efforts were prioritized within the budget available, and actions were often taken sequentially, thereby diminishing speed to regulatory approval and delivery. There were limited resources to mitigate risks by diversifying manufacturing outside of India, and some manufacturing investment offers were declined due to dose prices that were lower than high-income countries but higher than historic childhood vaccine prices.
Recommendations
As the global community considers next steps as well as reforms and new mechanisms to better prepare for pandemic risks, our review identified key recommendations:
In the near-term:
-
RDMIC and CEPI have a crucial role to play in developing better versions of existing vaccines to serve lower-income country access requirements (e.g., addressing thermostability, costs, ease of production and delivery), defining a variant strategy, and further developing manufacturing capacity and addressing manufacturing bottlenecks. RDMIC investments can provide major value added to (i) set standards for suppliers, (ii) incentivize manufacturing innovations for speed, cost savings, or reliability, and (iii) partner to develop mRNA manufacturing platforms in different geographic areas. In addition, as only a sub-set of the vaccines developed have been WHO pre-qualified, more could be done on alignment with WHO prequalification processes and SRA activities to assure parallel rather than sequential reviews.
In the future:
-
To meet access goals rapidly in the future, R&D funding should link with regulatory, manufacturing, and supply chain investments, bundled together under a framework agreement to enable insight and leverage with portfolio companies to ensure delivery. If a global mechanism is mobilised in the future (a successor to COVAX), investment in R&D and manufacturing needs to be simultaneous and coupled with access commitments and procurement through advanced purchase agreements.
-
Adequate financing is required even if the mandate is restricted to the lowest-income countries; callable capital facilities should be built to deploy to the COVAX successor when a pandemic-potential outbreak hits, with ex ante agreements in place on structure and governance of uses. The regional window of the World Bank’s IDA is a potential source if the appropriate mechanisms are in place, and if donors adequately recapitalize the facility.
-
CEPI itself should consider options for its role in the future of pandemic preparedness and response. Consider whether CEPI could become a one-stop shop in the future, including early procurement, or whether CEPI should be the articulating point around which regional entities such as BARDA and HERA – with analogous entities being stood up to cover other geographic regions – operate, with CEPI playing a global networking, coordinating and advisory role.
-
Requirements for future pandemic R&D are lessened with adequate intra-pandemic R&D and manufacturing investment as the CEPI 2.0 strategy lays out. Future funding of vaccines should target vaccines against multiple major respiratory pathogens as well as pancoronavirus vaccines. Funding is also needed for development of manufacturing innovations so that vaccines can be produced cheaper, faster, and closer to an outbreak, including investment in geographically diversified global manufacturing capability to enable more equitable distribution and accessibility of doses.
Disclaimer
CGD blog posts reflect the views of the authors, drawing on prior research and experience in their areas of expertise. CGD is a nonpartisan, independent organization and does not take institutional positions.



