Recommended


Blog Post
The World Bank’s International Development Association (IDA), the largest single source of concessional financing for development in lower-income countries, is under-utilized in the world’s fight against pandemics, and can deploy its resources and expertise to play a much more significant role in the COVID-19 response and beyond as part of its upcoming replenishment, known as IDA20.
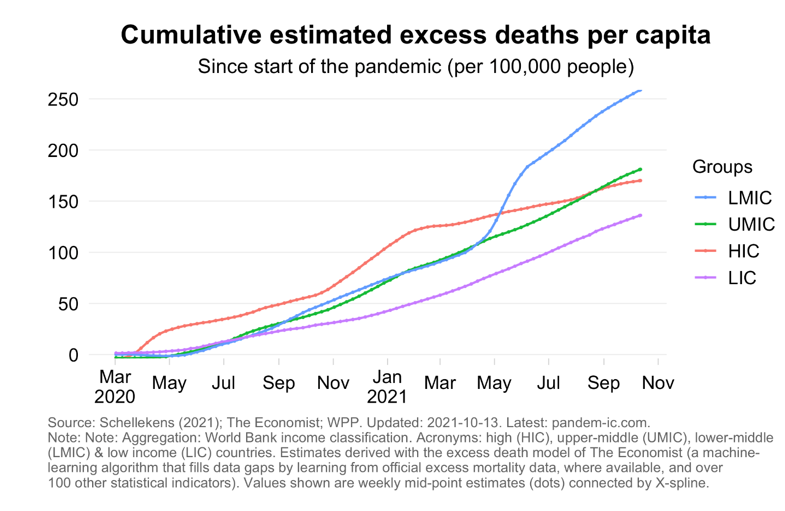
We can only avoid future pandemics—and end the current one, whose effects are now concentrated in lower-income countries (see Philip Schellekens’ graphic on cumulative excess deaths per capita below)—if we invest substantially more than in the past.
IDA19 commitments relating to pandemic preparedness (2020-23) are said to have “exceeded their original targets,” according to the World Bank’s own report. Yet whatever the formal commitment made under IDA19, the policy intent has surely failed given the scale of preventable excess mortality alongside a 4% vaccination rate in low-income countries, and the gross underreporting of cases and deaths. The current IDA20 documents bury the health response to COVID-19 under multiple sub-headings, maintain the narrow country focus, and preparedness for the next pandemic is a seventh order objective under the “human capital” title, even while the COVID-19 catastrophe has macro, governance, and broader sustainable development consequences. Worse still, the IDA20 policy commitment is almost identical to the commitment made under IDA19 despite everything that COVID-19 has wrought on lives and economies; “support 20 IDA countries with OneHealth approaches” sounds about the same as the IDA19 goal of supporting “at least 25 IDA countries to implement pandemic preparedness plans.” With 75 IDA-eligible countries, we can expect the next outbreak before most countries complete planning under these unambitious goals.
In the lead-up to IDA20, IDA donors must ask for much more on the immediate response as well as future pandemic prevention and preparedness. A stronger IDA20 on pandemic prevention and preparedness is an essential complement to the new proposal for a Global Health Threats Fund (GHTF) by the G20-commissioned High Level Independent Panel for Financing the Global Commons for Pandemic Preparedness and Response. One cannot work without the other—because the potential GHTF’s scope is restricted to global public goods that require non-ODA grant financing, because many national actions in global health security are high return investments for borrowing member countries themselves, and because the needs are so great that grant funding alone cannot hope to cover all resource requirements. A worst-case scenario would be to treat pandemic prevention and preparedness as outside or incidental to the IDA mandate, missing the needed engagement with lower-income countries’ policies and budgets, and creating the conditions for a rerun of COVID-19.
To address these omissions, I propose four IDA20 measures to strengthen the COVID-19 health response and to prevent and prepare for the next threat:
1. Establish focused management for rapid COVID-19 vaccine delivery and preparedness investments
The IDA-20 Special Theme: Human Capital document (paragraph 27) lays out a list of activities to include in country operations in support of COVID-19 vaccination rollout alongside health system strengthening and pandemic preparedness. While this country-by-country lending is vital, IDA funders should ask the Bank for a managerial structure that responds to the need for a more hands-on and regional approach to supply constraints and the imperative for rapid vaccination, as well as urgent investments in surveillance.
In April and October 2020, the World Bank Board approved up to $12 billion under the Global COVID-19 Multiphase Programmatic Approach (MPA for short) to support the COVID-19 health response, and later the acquisition and distribution of vaccines. The MPA did not modify total resources available to countries under their IDA envelopes (which meant that countries had to trade-off purchases of vaccines against other development investments) but did establish a fast-track process to approve operations and set up a “Bank-wide, dedicated corporate COVID-19 Task Force and HNP Practice Emergency Operations Center, overseen by a Bank-wide Steering Committee” (including but going beyond the health sector). In June 2021, President Malpass announced an additional $8 billion for vaccine financing, for a total of $20 billion. However, as of the end of September 2021, the Bank had only approved operations to support vaccine rollout for $5.8 billion, or less than a third of the funding available. About 250 million doses have been financed, of which half are expected for delivery within the calendar year.
It is time for an update of the approach to reflect changing circumstances. It is not just more money on offer that will speed vaccination and enhance surveillance, but instead the combination of resources only available at the World Bank that brings financing together with technical expertise and coordination with other agencies like WHO, UNICEF, Africa CDC, and others to move vaccination coverage more quickly. The Bank’s own October 2020 document lays out the challenges clearly, but has yet to report on the progress made:
An intense focus on expanding immunization capacity will be required, and countries must ensure that their health systems can effectively implement a comprehensive COVID-19 vaccine deployment strategy. This includes functional, end-to-end supply chain and logistics management systems for effective vaccine storage, handling, and stock management; rigorous cold chain control; robust service and coverage tracking systems; well trained, motivated and supervised vaccinators, tailored large-scale communication and outreach campaigns at household, community and national level; people-centered service delivery models that reach different target populations effectively; and effective political leadership. Countries will also need to consider and put in place any needed institutional frameworks for the safe and effective deployment of vaccines, including around ensuring voluntary vaccination practices; regulatory standards for vaccine quality; guidelines for acceptable minimum standards for vaccine management including cold chain infrastructure; and policies to ensure robust governance, accountability, and citizen engagement mechanisms.
Building on the MPA as well as previous experiences in the 2005-13 avian flu response, the World Bank should establish a “Global Program for COVID-19 Control and Pandemic Preparedness” to: (i) further incentivize vaccine and preparedness financing through IDA’s Regional Window; (ii) leverage and tighten coordination with other global and bilateral funding, including through country platforms, to ensure complementarity and drive robust responses and timelines for vaccine supply chains and vaccine delivery; (iii) use trust fund resources to run regional or national programs to co-finance vaccine delivery and other COVID-19 control actions via non-governmental entities where relevant (as in fragile states, for example, or areas underserved by government providers); (iv) jointly with the UN and other partners, regularly report on results as well as expenditure; (v) develop economic analyses to guide responses (on levels of vaccination necessary, on procurement of vaccine, on delivery of vaccine, on financing of preparedness, on investment in and subsidies for local or regional manufacturing, etc.); and (vi) urgently develop operations to scale up vaccination as well as surveillance completeness, accuracy, timeliness, and public availability, building and expanding on REDISSE–a lending program co-financed with donations that currently operates in 14 countries.
The new program should represent its own IDA20 special theme, recognizing that pandemic prevention, preparedness, and response merit the same level of policy and investment attention as climate change, and certainly has extremely high near-term human and economic costs over the IDA20 period if not more effectively mitigated.
2. Enable at-risk pooled advance purchasing of medical countermeasures during outbreaks
The World Bank did not join early efforts to finance and reserve vaccines for low-income countries, with the result that COVAX and bilateral orders came late and were caught up in the global rush to market that edged out deliveries to low-income countries. The pace of vaccination and pandemic outcomes would surely have been different if the Bank had provided a guarantee or direct resourcing to reserve COVID-19 vaccine before stage III trials concluded, and could have participated more actively in COVAX to diversify manufacturing and make other related investments, acting as an Operation Warp Speed for the world alongside CEPI, Gavi and WHO. IDA has flexibility in what it finances and, in the past, has supported international organizations without beneficiary governments’ guarantee (Africa Trade Insurance would be an example).
Most unfortunately, we are repeating the same situation with possible COVID-19 treatments where no pre-arranged financing is in place to reserve doses for low-income countries despite the huge number of excess deaths. Likewise, if there are COVID-19 vaccine-evading variants that require a new vaccine, there will be yet another rush on the market for which global institutions are neither prepared nor financed to address. And there could be a new pandemic threat—a pandemic influenza for example.
While it is possible to argue that COVAX or AVATT should be financed by bilateral aid and philanthropy only, there are high returns to country governments’ investments in this area and it will make sound economic sense to co-finance these purchases if they are necessary, or in response to new pandemic-potential pathogens.
The Bank should immediately develop policies and protocols to facilitate early at-risk purchases when pandemic-potential outbreaks arise, and if needed a financing instrument--ideally backed by IDA donor guarantees in case country demand does not materialize--that would enable these at-risk purchases via a set of pre-approved organizations like Gavi, CEPI, AVATT, UNICEF, Global Fund, PAHO Strategic Fund, or others.
3. Set clearer IDA20 policy commitments for pandemic preparedness
IDA20 should strengthen its policy commitments on pandemic prevention and preparedness beyond the currently proposed goal. These actions would not only serve to reduce pandemic risk (through prevention and preparedness) but would also mitigate related threats, including antimicrobial resistance, and improve country capacities to reduce ongoing disease burdens from both infectious and non-communicable diseases. Options to consider include:
-
Work with WHO, OIE, and other partners to conduct and improve joint external evaluations of the International Health Regulations and Performance of Veterinary Services assessments in all IDA countries to lay out preparedness needs/gaps and financing scenarios, define the role for IDA and related financing, and feed into National Action Plans for Health Security (NAPHS). Financing for the investments identified through the assessments should be a priority within IDA lending.
-
Set a goal for IDA countries, consistent with their international commitments, such as: “By 2030, at least 80% of all countries’ veterinary and human public health systems meet international standards.” Consider making other kinds of IDA operations conditional on adequate progress towards these standards.
-
Approve a Pandemic Preparedness Action Plan for the World Bank Group including IDA commitments, building on the experience of the Climate Change Action Plans, including country coverage and finance targets for overall flows.
-
Assure that Country Economic Memoranda, Poverty Assessments, Public Expenditure Reviews, and Systematic Country Diagnostics identify key challenges related to pandemic prevention and preparedness and identify opportunities for countries to accelerate progress towards this objective.
-
Report on spending on core public health functions, work with the IMF to create a new reporting line in IMF GFS for expenditures on key public health functions.
Whatever options are included, it is important that this area not be treated as a “tick box exercise” as is the current situation (20 countries with a plan, yes or no). The aim is that Bank operations in relevant areas (but especially in health) routinely include health security and preparedness in the same way that Bank projects generally support maternal and child health, or actions to promote universal health coverage.
4. Strengthen lending and trust fund incentives for greater financing and progress
Financing plays a role in breaking the entrenched patters of underinvestment, and in countering the many disincentives with clear requirements and incentives to take responsibility for prevention and preparedness. This needs to be intentionally built into funding, financing instruments, and packages. While also relevant for IBRD clients, in the context of IDA, IDA donors should:
-
Assure that borrowing for core public health and preparedness is at least partially additional to IDA’s performance-based allocations or country envelopes. In addition, it would be possible to add more overall concessional resources and reserve a share of regional IDA for this purpose.
-
Use trust fund resources or other external monies to finance project preparation facilities to build pipeline for core public health system investments and to ensure adequate funding of the requisite technical assistance from WHO and OIE, among others.
-
From similar sources, align other bilateral and multilateral funders within the IDA operations, potentially to co-finance lending operations as in the Global Financing Facility.
-
Create incentives for needed policy reforms or progress using policy-based, results-based, and/or programmatic lending instruments.
-
Obtain semi-annual reports on implementation progress of the NAPHS, including number of countries with NAPHS that have financing shortfalls and rationale for IDA not filling the gap.
-
Update Country Policy and Institutional Assessments (CPIA), which form part of IDA’s funding allocation formula, to reflect countries’ preparedness stance.
If donors ask more from IDA, it is reasonable that IDA must ask more from donors. There are already admirable plans to stretch the balance sheet to lend more and talk of rechanneling SDR, but greater concessional resources remain vitally important. Shareholders must support a timely and appropriately sized replenishment of IDA to ensure that the greater focus on pandemic response and preparedness is not at the expense of poverty reduction.
Disclaimer
CGD blog posts reflect the views of the authors, drawing on prior research and experience in their areas of expertise. CGD is a nonpartisan, independent organization and does not take institutional positions.
Image credit for social media/web: Adobe Stock




{kind=link}