Recommended

Twenty months into the COVID-19 pandemic, there is broad agreement that more and smarter international financing is needed to respond to the current pandemic and to prepare for the next global health threat. Most estimates of international financing needs have converged around a $50 billion immediate requirement to respond to and control this pandemic and a $10 billion annual requirement for sustained preparedness. There is also consensus that these requirements should be funded multilaterally for the collective or common good and avoid zero sum trade-offs in the use of aid for other global health or wider development priorities of equal importance. The G20 independent panel report and this blog, among others, highlight the priorities for the uses and needed characteristics of the funding, but now to the next hard question – how to raise the money?
What are the sources of revenue beyond ODA that could contribute to the proposed Global Health Threats Fund?
A first premise is that most governments do and should self-finance pandemic preparedness and crisis response with their own domestic resources. The G20 Independent Panel (HLIP) estimated that low- and middle-income countries should aim to increase domestic health spending by 1 percent of GDP over the next five years. High income countries will also need to increase their domestic investments, around $15 billion over the next 5 years according to HLIP. Much of this spending has direct domestic benefits and is highly cost-effective given national budget constraints and priorities.
But increased domestic spending will not be enough to meet the pandemic threat. There must also be adequate financing for actions that benefit neighboring countries and the entire world such as research and development of medical countermeasures, ever warm and distributed countermeasure manufacturing and stockpiling as well as global and regional efforts on pathogen and disease surveillance. International financing is also needed to support public good elements of investments in lower-income countries as they face intensely competing demands amid very scarce public budgets for the foreseeable future.
Like all ambitious collective actions, there will and must be multiple sources of finance including but ideally minimizing the use of ODA whose principal purpose is to meet national development priorities in developing countries. That said, money is fungible – the budgetary source or coding of monies is ultimately an artificial designation and money will come from country governments, firms, philanthropies, or populations in one form or another. The aim is to assure that the benefits far outweigh the costs of this necessary investment; forthcoming work by Alessandra Løchen and colleagues at Imperial College London puts the returns to pandemic preparedness in four countries studied at 2-25 percent of GDP depending on the type of pathogen that is controlled.
To raise the estimated $10 billion a year required, there are several, complementary strategies needed to build a sustainable base for preparedness and response going forward:
-
Fair share finance: This strategy would form the core of a new financing mechanism – raising finance via an agreed global burden sharing formula where each country contributes according to the size of their economy and population, building on the principle of collective defense and common funding as in the core funding of the UN and WHO or the direct funding of NATO maintenance and crisis response. Such an approach was proposed for the finance of ACT-A (Financing Global Health Security Fairly | Center For Global Development); some progress has been made but many higher-income countries have not yet contributed a fair share (see WHO covid funding tracker exposes most donors’ lack of willingness to pay | Development Today). Draft bipartisan legislation circulating in the US Congress includes a proposal for a multilateral financing mechanism where “fair share” financing is encouragingly part of the package. The European Council has also issued a joint statement that the EU will contribute its fair share to ACT-A thereby also implicitly supporting such a process.
-
MDB finance: The G20 HLIP report suggested that a share of global health security financing be raised and leveraged via the World Bank:
-
For low-income countries, stretch IDA balance sheet to lend more (for example: More Than $1 Trillion in MDB Firepower Exists as We Approach a COVID-19 “Break the Glass” Moment | Center For Global Development)
-
For middle-income countries, leverage small amounts of donor grant funding to obtain greater lending volumes and/or to buy-down IBRD lending terms using International Financing Facility for Education (IFFEd) type approaches (worked example here: Annex I | Pandemic Financing)
-
Expand lending volumes or adjust lending terms based off interest generated from a reserve allocation of SDR to IBRD and IDA who are authorized SDR-holders (as in the IMF’s Poverty Reduction and Growth Trust Three Ways New SDRs Can Support the IMF’s Lending to Low-income Countries | Center For Global Development)
-
Deploy IBRD net income and IDA repayments into a general global public goods fund (as done previously in 2018 but less since), building on differential or flexible pricing of IBRD loans according to country income status (see: On Global Public Goods: It’s Not Big Money but It’s a Big Breakthrough | Center For Global Development)
-
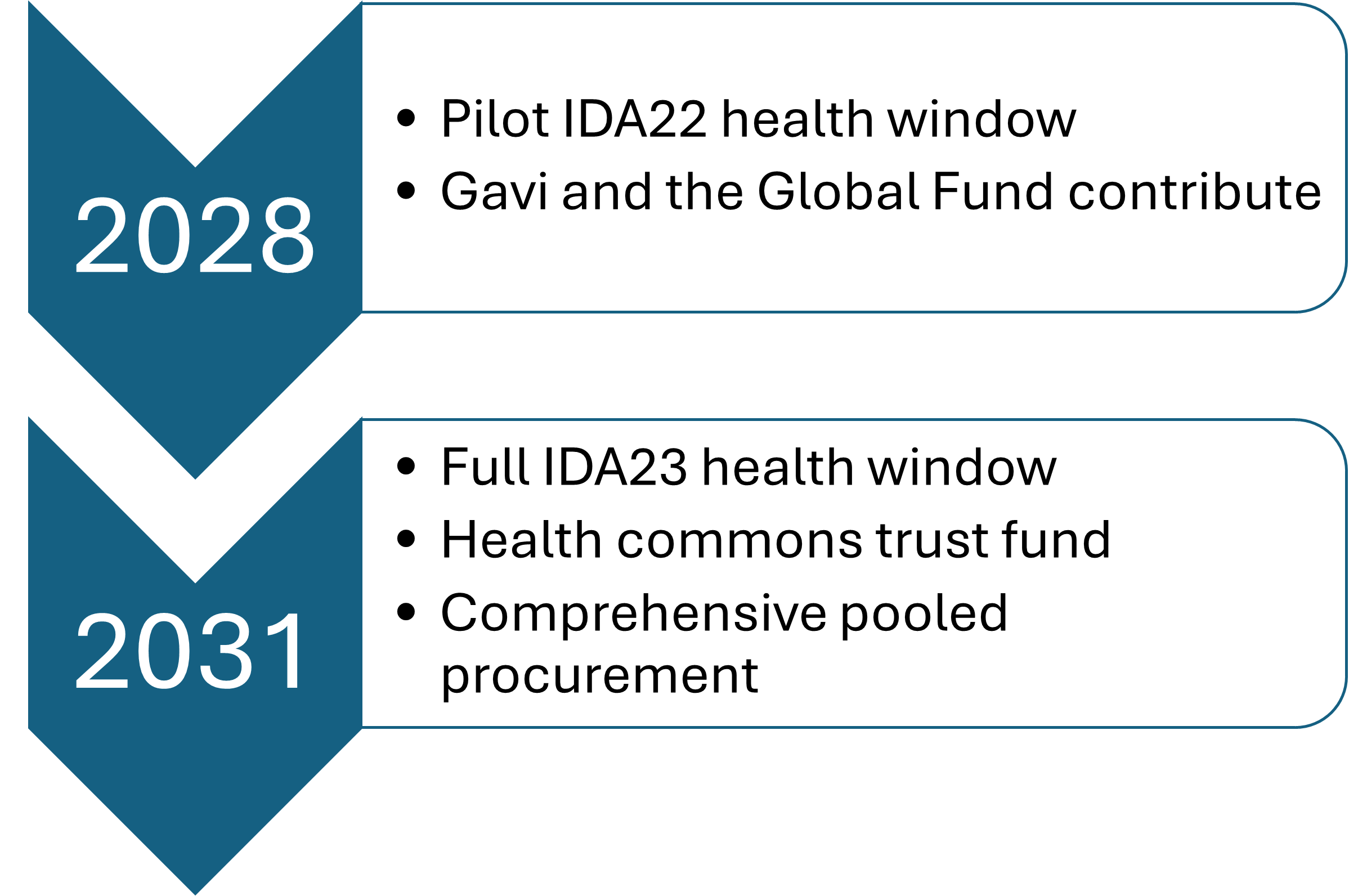
Build a dedicated pandemic preparedness window into a larger IDA20 replenishment; while IDA contributions are generally classified as ODA, resources are leveraged and on lent under highly concessional terms (Realizing the Crisis Preparedness and Response Ambition of IDA20 — Centre For Disaster Protection; IDA-20: Donors Must Go Big, and IDA Must Too | Center For Global Development)
-
-
International Finance Facility (IFF) outside the World Bank: The G20 HLIP suggested a version of an IFF that could leverage greater volumes of lending via the World Bank. Another option, proposed by the Independent Panel, is an IFF modeled on the IFF for Immunization that is run as a special purpose vehicle and independent organization operating to provide financing to Gavi, the Vaccine Alliance. This idea is summarized here: Panel paper 14 - Financing ERCE)
-
Pandemic super-profits levy: Institute a temporary surcharge on multinational firms that have experienced large profit growth during the pandemic, using the proceeds to finance COVID-19 response and recovery contributions and pandemic preparedness (for example: A COVID-19 Recovery Contribution – IMF Blog)
-
Global health security fees: Enact small national fees or levies on international travel, transactions, or commerce to assure global health security given these activities’ contribution to the rapid spread of pathogens akin to the “September 11 Security Fee” that finances the US Transportation Security Administration’s work to make airports safer, or the national airline tax levy that was earmarked to finance UNITAID.
-
Eliminating or reducing duty-free sales (starting with tobacco) and earmarking proceeds: Eliminate or reduce duty free sales in airports, starting with tobacco, and use to help fund; CGD estimates that eliminating duty free sales/imports would raise about $7 billion a year in revenues as well as reducing consumption of tobacco and therefore risk factors for COVID-19 among other diseases (see: Eliminating Duty-free Tobacco—What Went Wrong? | Center For Global Development). This measure was already agreed in an international treaty (the Framework Convention on Tobacco Control) but not yet implemented.
-
Drawing finance from defense budgets, for example, by creating a “Health Defense Operations” designation in US budgets (and equivalent elsewhere) to protect from budget caps (HDO).
-
Philanthropic and private contributions: Much of existing global health funding is sourced from philanthropy. As preparedness actions are the quintessential global public good, it is fitting that governments are the main architects and sources of finance. However, philanthropic and other kinds of contributions could be considered as start-up or seed funding.
New financing for global health security needs to be mobilized and invested now to respond to COVID-19, to strengthen the fight against all infectious diseases, and to prepare for the next pandemic threat. Surveillance investments at global, regional, and country level are needed immediately to build speedier and more complete mortality registration; extend the coverage and quality of testing, case detection and follow up; and further develop genomic surveillance capacity, as set out in the G7 plan. Similarly, the investment in R&D as well as manufacturing platforms that would speed the deployment of variant-specific vaccines or vaccines that could provide broader protection against coronaviruses would help with the current response as well as mitigate future pandemic risks.
DISCLAIMER & PERMISSIONS
CGD's publications reflect the views of the authors, drawing on prior research and experience in their areas of expertise. CGD is a nonpartisan, independent organization and does not take institutional positions. You may use and disseminate CGD's publications under these conditions.