May 12, 2010
On Sunday the New York Times published four article on the battle against AIDS in Uganda which everyone should read who is interested in the AIDS epidemic, or in the effectiveness of US aid policy in general. The articles, all by the Times’ knowledgeable science reporter and long-time observer of the AIDS epidemic DonMcNeil, include:
- At Front Lines, AIDS War Is Falling Apart
- After Long Scientific Search, Still No Cure for AIDS
- As the Need Grows, the Money for AIDS Runs Far Short
- Cultural Attitudes and Rumors Are Lasting Obstacles to Safe Sex
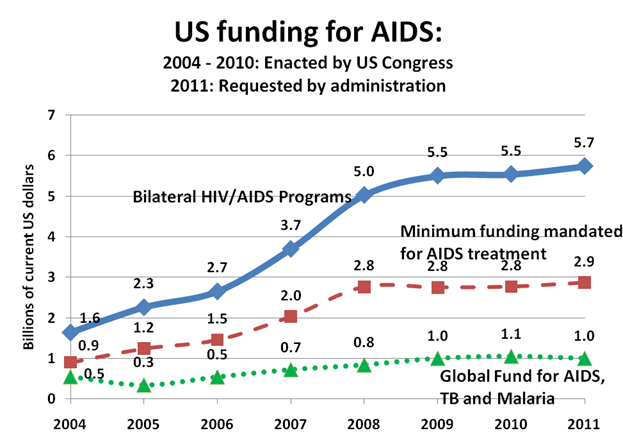
Figure 1. After growing at 25 % per year for 2004 – 2008, PEPFAR funding has grown at less than 5 % per year since 2008 and the mandated expenditure on AIDS treatment is constant since 2008. (Source: http://www.pepfar.gov/documents/organization/80161.pdf accessed April 25, 2010.)
When the total amount of PEPFAR support stops growing, US personnel and their partners in countries like Uganda must make hard decisions. As long as they respect the entitlement of existing AIDS patients, every other part of the AIDS budget will be squeezed. So the potentially available money to add new AIDS patients to the treatment rolls, as well as money for HIV prevention and care for orphans – and newly mandated efforts to strengthen domestic health provider training, etc. - will ALL be squeezed. But this doesn’t mean that AIDS treatment is falling apart. It’s the INCREASE in the number of patients on treatment that has been SLOWED – and even apparently frozen in some clinics. Don McNeil’s article on treatment is misleading in another respect. It implies that the human tragedies it recounts that occur when people are turned away from treatment are only now appearing for the first time in Uganda. But for the last several years, despite the rapid acceleration of AIDS treatment access in Uganda, AIDS patients have been dying every year before they could find a treatment slot in a clinic. In fact for recent years less than a quarter of those estimated to be in desperate need of treatment actually received it each year. The latest data from UNAIDS estimates AIDS deaths to have been 77,000 in 2007. Increased treatment availability has reduced this number since 2007, but we estimate there to have been about 50,000 AIDS deaths in 2009. So the fact that people are dying of AIDS in Uganda is not new and should not be used to characterize the effort as “falling apart”. The article on prevention is also misleading because it implies (1) that Uganda was previously a good example of how to do everything possible to prevent HIV and that (2) people have recently reverted back to the risky behavior of the past. On the first point, Uganda has definitely NOT made a serious effort with every possible promising HIV prevention intervention. It has not scaled up male circumcision or widely expanded couples counseling, two widely advocated promising interventions supported by evidence. Even more shocking, Uganda has never attempted to invent an African version of Thailand’s “100 % condom program” to assure that a condom is used on 100 % of the riskiest sexual encounters. The first step in such a program would be to establish a nationwide inventory of all the bars, truck stops, and other “hot spots” where people meet in search of romantic relationships. The research on the so-called PLACE method, invented by University of North Carolina researchers ten years ago and described here, is the first place for an African leader to look who really cares about HIV prevention. Why wasn’t this program rolled out ten years ago in Uganda? The reasons are many and include the US government’s obsession with the A (abstinence) and B (be-faithful) parts of the ABC prevention program. But part of the blame goes to those on the left of the political spectrum, so worried about the human rights of potentially stigmatized people with high risk behavior and the vulnerability of monogamous women that they insisted prevention efforts be diluted over the entire population – instead of focused on those contributing the most new infections as would have been possible using the PLACE method. Has the behavior of Ugandans reverted? In one sense, yes, since HIV infection rates have risen among young women at some ante-natal clinics and self reported risky behavior has also risen. Perhaps this is due to complacency due to the widespread availability of free and effective AIDS treatment. However, despite my record of warning of such a possibility, there is no evidence that this “disinhibition” has yet occurred in Uganda. Instead it seems likely that part of the decline in prevalence and increase in risk behavior has been due to the deaths of those with the riskiest behavior, who were not lucky enough to get onto treatment. Their removal from the population would automatically reduce both prevalence and reported risk behavior. As a new cohort matures and becomes vulnerable to AIDS, it would not be surprising if the same percentage have unusually risky behavior as was the case a generation ago. So the rise in prevalence in risky behavior might be due to the arrival of a new younger cohort of vulnerable people and not to the same people who were practicing safe sex, changing their behavior and reverting to risky behavior, as the article implies. Despite these misleading aspects of the NYT articles, the facts call out for a new way of thinking about the AIDS epidemic. Failure to sustain the promise of treatment was inevitable as long as the number of new infections remained high. The financial crisis has only slightly advanced that terrible day of reckoning. The international community has got itself into a terrible dilemma: treatment for AIDS is already consuming resources that could be used much more effectively to stop other killer diseases, like childhood diarrhea, and yet millions still lack access to treatment. If we can’t treat everybody, what should we aim to do? Increasing AIDS funding, even if practical, will never be enough by itself to stem the epidemic. (For contrary views, see here and Gregg Gonsalves’ comment here. ) We must shift now to achieve an AIDS Transition: invest massively in prevention to reduce the number of new infections, so that, eventually, we will be able to attain high levels of treatment coverage AND have a declining number of people who are infected with HIV. The idea of an AIDS transition is explained more fully in the first of a series of essays I will release next week.Topics
DISCLAIMER & PERMISSIONS
CGD's publications reflect the views of the authors, drawing on prior research and experience in their areas of expertise. CGD is a nonpartisan, independent organization and does not take institutional positions. You may use and disseminate CGD's publications under these conditions.



