Recommended

Event
In a May appearance on 60 Minutes, US Federal Reserve Chair Jerome Powell stated that “the thing that matters more than anything else is the medical metrics, frankly.” Powell was referring to the need to closely track deaths to understand the trajectory of the COVID-19 pandemic and its effects on the economy and well-being. Indeed, authors at the Cleveland Fed were tasked with assessing which mortality statistics would best reflect reality. Remarkable from the nation’s top economic decision-makers given their usual focus on measures like productivity and inflation, and an insight that now holds true for the entire world–measuring deaths completely, accurately, and quickly is an essential prerequisite to better economic and public health policies during COVID-19 and beyond.
Yet despite its centrality to our collective fates, the state of mortality reporting is dire. Most low- and even middle-income regions lack data on deaths (see figure 1). How is it possible to assess whether sub-Saharan African countries are winning the fight against COVID-19 if more than 70 percent of total deaths in a non-COVID year go unreported? Or how to judge the likely trajectory of Pakistan during COVID-19 if no mortality data of any kind is reported in the public domain, according to the World Health Organization’s (WHO) 2019 mortality report?
Figure 1. Availability of deaths by completeness status and region
(2010-2015; UNSD/Skenderi 2016)
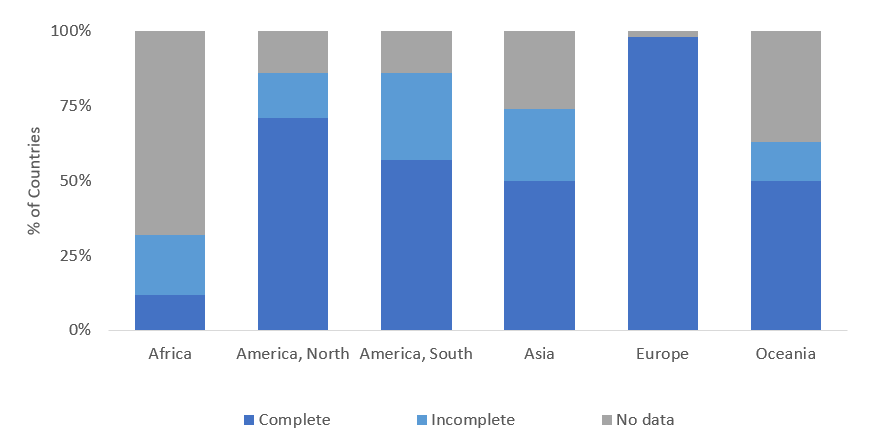
Perhaps most troubling: mortality reporting has remained poor despite decades of US and other wealthy country investment in global health programs to combat other infectious diseases like HIV/AIDS, malaria, and Ebola, among others. Cause of death data is complete in only 6 percent of African countries and 10 percent of Southeast Asia, according to the UN’s Statistical Division. As Matthew Kavanaugh, Ingrid Katz, and Charles Holmes recently pointed out: “the absence of data on actual mortality at the program and clinic level, whether all-cause mortality or AIDS-related mortality, has undermined the AIDS response on several fronts.” Even hospital statistics on cause of death cannot be assumed to be correct according to Rasika Rampatige and co-authors in 2014. And there is no data to be found on timelines and lags associated with mortality reporting outside of high-income countries.
Academics have often documented the problem over the years. But to date, global health funder response has been fragmented, directed exclusively to the deaths of infants and children, and insufficiently scaled.
The US Agency for International Development’s funding of the Demographic and Health Surveys has helped to generate high-quality (though infrequent) measures of infant and child mortality over the years, and later maternal mortality. Demographic surveillance sites were launched in different locations in sub-Saharan Africa and South East Asia, again with a focus on child deaths. But none of these efforts provided systemic support for routine reporting of deaths and cause of death that would include the entire population, despite good ideas for low-cost systems.
In response to this omission, in 2014, the World Bank and WHO launched an investment plan to improve CRVS in low- and middle-income countries. Since that time, more meetings were held at the UN Statistics Division with partners, a center of excellence was created at IDRC-Canada, an e-learning course is in place at World Bank, WHO published a resource kit and a regional strategy in South East Asia, the Economic Commission for Latin America and the Caribbean formed a project, the Government of Canada granted funding to the Global Financing Facility for civil registration and vital statistics (CRVS) strengthening, and Bloomberg Philanthropies launched a Data for Health Initiative with supporting grants to Vital Strategies and others.
All these have been important developments, but none have yet transformed the situation of mortality reporting and are mostly at the scale of limited technical assistance rather than the massive investment that improved mortality data deserves, given its macro-criticality to COVID-19 recovery and the rest of the global health enterprise. And few have placed these investments in the context of pandemic preparedness–external evaluations of preparedness include laundry lists of hundreds of indicators but mortality data accuracy, completeness, and speed are not among them.
Today, we’ll hold an online event to kick off a conversation and agenda on low-cost, high-impact strategies to collect better quality mortality data in real-time, and country experiences to date with Philip Setel and Fatima Marinho from Vital Strategies, as well as Samira Asma of WHO and Erin Nichols of the US Centers for Disease Control and Prevention. Next week, my colleague Damian Walker will follow with a blog on the role of mortality data in assessing progress in COVID-19 control. Ideas welcome.
Disclaimer
CGD blog posts reflect the views of the authors, drawing on prior research and experience in their areas of expertise. CGD is a nonpartisan, independent organization and does not take institutional positions.


