Recommended
With oxygen on tap, India need never get asphyxiated again.
Since January 2020 the world has been grappling with the COVID-19 pandemic in waves of varying severity. Still, oxygen is the sole therapy for managing COVID-19-induced hypoxaemia, an abnormally low level of oxygen in the blood arising from diverse life-threatening lung conditions. As blood oxygen levels fall, organs and tissues begin to fail, and patients with severe COVID-19 must be urgently placed on supplemental oxygen.
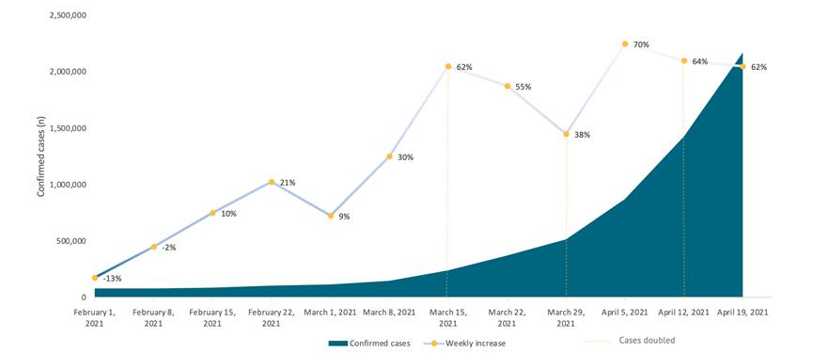
A devastating second wave of coronavirus across India saw the daily demand for supplemental medical oxygen rising to roughly 12 times what was needed pre-COVID-19 times, with a catastrophic impact during March, April, and early May, 2021. The health sector, so long neglected with chronic under investment, was simply unable to speedily ramp up critical care, to provide oxygenated hospital beds, ICUs, medicines, and ventilators, much less back up supplies. Demand for oxygen far exceeded the immediate availability, and existing hospitals and crematoriums were completely swamped and overwhelmed. Some state governments, however, notably Kerala, had planned in advance, and overall maintained a surplus of oxygen.
Most oxygen disasters across India could have been avoided.
Most oxygen disasters across India could have been avoided. This blog describes the current model of medical oxygen supply in India, outlines the response to the oxygen crises, including the problem of severe oxygen shortages in some Indian states, and provides recommendations on how India could prevent the next crisis stemming from shortages in oxygen.
What is the current model of medical oxygen supply?
In India, medical oxygen is currently sourced by both private and government hospitals through the market. During “peacetime”, i.e. in periods of normal and only slightly fluctuating day-to-day demand, this mechanism works reasonably well, except where serious governance deficits exist, (as in Gorakhpur). However, in the face of a ferocious and widespread pandemic, market mechanisms without adequate safeguards and stewardship lead to perverse outcomes. Because supplies are fixed in the very short term, prices may rise manifold, making oxygen unaffordable and leading to a high mortality rate among the very poor. Other outcomes could include hoarding in anticipation of future price rises, actions that would lead to that same outcome. Sadly, we have witnessed all of this.
Additionally, there are problems of geography and logistics. Cryogenic liquid oxygen for medical use is produced off-site, mostly concentrated in eastern India, at 4000MT per day. The unprecedented numbers of preventable oxygen starvation deaths during the COVID-19 pandemic have highlighted that the current model of obtaining medical oxygen is unsound and dysfunctional.
What led to the problem of severe oxygen shortages in some Indian states?
During the COVID-19 crisis, India required about 8000 metric tonnes of medical oxygen per day, so the central government sought to supplant the market with a hastily conjured system. The distribution of available medical oxygen supplies was taken over by the central government, while a significant percentage of industrial oxygen was diverted towards higher supply of medical oxygen, and exports were banned. Industrial oxygen—up to an additional 6000 MT per day—was diverted for medical use, being the combined output from steel plants and oil refineries in Odisha, West Bengal, Chhattisgarh, Karnataka, Tamil Nadu, Haryana, Mandi Gobindgarh in Punjab (while the plant in Goa was made functional).
The allocations of oxygen to the different states were determined on the basis of some formula related to the numbers of oxygen beds and ICU beds. In this model, the states, in turn, would arrange distribution to public and private hospitals within their jurisdictions. The basis for such distributions initially remained unclear. The second wave of COVID-19 crested in different states at different times, and the over-centralised response and use of a rigid formula for allocations lacked flexibility. It failed to track and take account of the varying incidence of COVID-19 infections, hospitalizations, and near death emergencies. The Medical College Hospital in Bambolim, Goa, for instance, would depend upon a faceless authority in the government to determine state-wide “allocations” of oxygen, which would, in turn, trickle down from state level authorities to individual hospitals. In the absence of proper planning, this was a recipe for bottlenecks, disaster, and deaths. Several states sent emergency SOS alerts and turned to high courts seeking emergency replenishment of oxygen supplies.
Transportation of liquid oxygen from the production sites to the rest of the country (in particular to cities in the north and west), by rail or trucks with cryogenic containers, takes up to 12 days. The interim periods between allocation and delivery of oxygen saw the demand for oxygen skyrocket. Initially, even the oxygen available did not get transported in time to where it was needed. Special cryogenic containers required to drive oxygen in large quantities across states fell short as well. These were not enough to move the entire oxygen production. Cryogenic containers were imported and the Indian air force and railways engaged in emergency operations to transport oxygen across the country. The government took measures to allow tankers on any roads, regardless of limitations like state-specific permits, giving them priority status similar to ambulances. There was also a shortage of cylinders, which were not being refilled fast enough to meet demands. Cylinder-filling facilities, too, are now allowed to operate 24-hours a day, seven days a week, and cylinders typically used for other gases, are (after appropriate sanitizing), being turned into oxygen containers. The government anticipates that by August 2021, the daily production of medical oxygen could cross up to 9,500 MT. After an April 2021 meeting of the Joint Plant Committee (JPC), Statistics Wing, Ministry of Steel, Government of India, “it may touch 10,000 [MT/day], if everything goes right,” was one optimistic refrain. However, it is impossible to say whether this would be adequate in a future medical emergency.
The government of India had solicited bids in 2020 to establish district-level 162 pressure swing adsorption (PSA) plants—facilities containing machines able to condense oxygen from the air—for government hospitals, but it took eight months to award this contract. At the time of writing this blog, only 33 PSA plants have been installed (and not all are functional) across 15 states, leaving most facilities dependent on external provision.
Our recommendation: the Nested Nodal Allocation Model (NNAM)
COVID-19 has made abundantly clear that, in an emergency, supplies of medical oxygen must be managed with advanced planning and rigorous monitoring, and cannot be left to the market. Planning for such emergencies is not easy, and there are at least three challenges:
- first, that it is difficult to predict the demand for oxygen at any level (national, state, district) that might arise in a future emergency,
- second, that logistics of distribution from the supply sources to state capitals, further to district headquarters, and still further to community and primary health centre levels are extremely difficult, and
- third, that information flow, and compliance with the directions of planning authorities, takes time.
We propose a response model that utilizes dynamic and evolving supply and demand information and is embedded within an agile, multi-level governance model for oxygen in times of crisis, such as the COVID-19 second wave, to replace reliance solely upon the market. We call this model the “Nested Nodal Allocation Model” (NNAM). It has 4 key elements.
1. Clear governance arrangements and protocols
During peacetime, district, state, and central NNAM authorities should be designated -- including composition, roles, and responsibilities -- and protocols are to be closely followed. Standard operating procedures on buffer stock, flow of information, and oxygen allocations should also be developed. For example, the District NNAM Authority must maintain at all times a buffer stock defined on the basis of a specified number of days of normal peacetime use, say 10 days.
The composition of the authorities at different levels could be as follows:
- District NNAM Authority: it may be chaired by the district collector, and it may include the district civil surgeon, a representative of the transport department, and the district level private hospitals.
- State NNAM Authority: it may be chaired by the principal secretary for health, and it may include the state Director of Health, a representative of the transport department, and state level private hospitals.
- Central NNAM Authority it would have a similar composition to the State NNAM Authority, and in addition, it might include a representative of medical oxygen suppliers.
2. Adequate supply including excess capacity built-in
As part of the preparatory work, there should be a mandate for adequate supply of oxygen at all licensed hospitals, public or private. This supply could come from installing, maintaining, and operating their own oxygen plants, strengthening liquid oxygen infrastructure when possible, and/or providing for stand-by oxygen concentrators and cylinders.
Large hospitals can produce oxygen on-site, which is typically done by PSA plants, from which oxygen is then piped directly to (oxygenated) beds. Indigenous technology for this purpose has been developed by the Defence Research and Development Organisation (DRDO), and made available at low cost to domestic manufacturers. Smaller hospitals, community and primary health centres will rely on portable oxygen concentrators and stand-by cylinders. The latter come from a network of small refilling stations located in every district.
Additionally, the NNAM mechanism should identify in advance the plants from where medical-grade oxygen (including by diversion from industrial sources) may be obtained, the compensation to be paid to these plants, and the infrastructure to manage the logistics during times of crisis. This identification process may involve substantial investment in redundant capacity, such as cryogenic vessels, and a conscious public decision in advance for the provision of necessary funding.. It should be recognized that such redundancy is a public good, and therefore a government responsibility. Such investment should come from the central budget to allow for a flexible and efficient allocation.
3. A clearinghouse with standardized flow of information on the demand and supply of oxygen at all levels
Once the NNAM is activated, each hospital should report everyday its demand for oxygen to a designated authority (we call it the “NNAM District Authority”) at the district level, shortfall over its own production, and the remaining buffer stock. Oxygen planning tools can help in calculating the projected demand. The district NNAM Authority would aggregate this information each day, specify the amount available in its own buffer stock, and submit the same to the designated state NNAM Authority. The state NNAM Authority would aggregate demands from the districts and communicate this information to the designated central NNAM Authority.
4. Top-down allocation and distribution of oxygen
Once the NNAM is activated, the Central NNAM Authority would be in charge of allocating the available oxygen supplies each day to the demanding states as per the norms adopted in advance, and further, would organize their delivery to the state capitals (or other identified major city). The state NNAM Authority would, in turn, re-allocate each day’s arrivals to the district NNAM authorities on the basis of advance norms, and organize the logistics of distribution. The district NNAM authorities, in turn, would do the same. At each level, information flows both upwards (demands) and downwards (allocations). The buffer stocks at each level serve to smoothen variations between demand and supply at each point in time.
Conclusion
It is important to emphasize that the model described above cannot easily be organized on the fly. Attempts to do so will result in the chaos that we have seen during the second wave of COVID-19. The government should put the system into place, train personel in operating the standard operating procedures, and practice dry-runs. Many countries have faced severe oxygen crises in the current pandemic. The planning model proposed here for India can be contextualized and applied to other low- and middle-income countries. No country needs to suffer like this ever again with the right investments and planning.
Meenakshi Datta Ghosh is a former Secretary of the Government of India, is now an independent development professional, specialising in the interface of governance, public health and public policy.
Aruna Sharma is a practitioner development economist and retired Secretary of the Government of India .
Disclaimer
CGD blog posts reflect the views of the authors, drawing on prior research and experience in their areas of expertise. CGD is a nonpartisan, independent organization and does not take institutional positions.



