
In a recent blog, we asked “what do we really know about COVID-19’s impact on essential health services?” In that blog, our focus was primarily on what international partners were doing to monitor the effects of COVID-19 on essential health services. What we didn’t highlight is the increasingly detailed evidence emerging from countries themselves, which paints a varied picture of national policy responses to the pandemic and the impacts of those responses.
CGD has partnered with local institutions in Kenya, the Philippines, South Africa, and Uganda to explore the indirect health effects of the pandemic in different ways and using different data sources. Over the coming months, we’ll be releasing that work in a series of working papers, as well as hosting a series of virtual events where the authors will share their findings. In this blog, we share some early results from the work in the Philippines: an analysis of claims data from the Philippine Health Insurance Corporation (or PhilHealth).
COVID-19 and the Philippines
The Philippines is one of the countries most affected by COVID-19 in the East Asia-Pacific region. The country has recorded 578,000 confirmed cases and 12,000 deaths as of March 2, 2021. As COVID-19 continues to spread, government leaders have focused on tracking COVID-19 cases, hospitalization, and deaths. In fact, the government has built an entire system to track these numbers. However, these numbers hardly capture the total harm caused by the pandemic and associated policy responses. As we have argued elsewhere, governments should capture both direct and indirect effects in order to have a holistic and calibrated public health response.
In the Philippines, anecdotes on the declining use of essential healthcare services are mounting, but compelling evidence remains scarce up to this day. Reports suggest that non-COVID-19 patients are deferring care because of dwindling healthcare resources; they are decreasing health visits because of mobility restrictions or fear of getting infected. The country remains under different levels of large-scale community quarantine since March 2020; schools are still closed, and children and high-risk individuals are not allowed to go out except for essential services.
As in many low- and middle-income countries, the limited and fragmented health information system in the Philippines makes tracking hospital admissions and health visits challenging. We have been analyzing claims reimbursement data to explore the indirect effects of the pandemic. We are also collecting data on hospital admissions and primary care visits directly from health facilities to triangulate our analysis of claims data.
Claims data from PhilHealth
The Philippine Health Insurance Corporation, or PhilHealth, is one of the primary government agencies implementing the country’s universal healthcare (UHC) program. Almost 90 percent of Filipinos are members of the program, and almost all of the 1,300 hospitals in the country submit health insurance claims to the service. Philhealth uses case rates to pay public and private healthcare providers. Each medical claim has a corresponding ICD10 code (a code assigned under the World Health Organization’s medical classification list) and Relative Value Scale code (a code used to generate fee schedules) for a procedural claim. It receives almost 12 million claims every year, amounting to USD1.9 billion. Given these, the PhilHealth’s claim data could be useful to demonstrate the extent of indirect effects of the pandemic on non-COVID patients.
We examined the health insurance claims of 12 diseases, which together account for approximately 50 percent of the total disease burden of the country (IHME, 2020). These diseases include stroke, cancer, gastroenteritis, pneumonia, chronic kidney disease, hypertension, chronic obstructive pulmonary disease (COPD), dengue fever, asthma, diabetes, ischemic heart disease, and tuberculosis.
Preliminary findings
Figure 1 shows the number of claims from 12 high-burden diseases. The precipitous decline in the number of medical claims during the pandemic occurred in both public and private health facilities. The number of claims has not returned to pre-pandemic levels in the third quarter of 2020.
Figure 1. Number of medical claims for high-burden diseases, Jan 2018 – Oct 2020
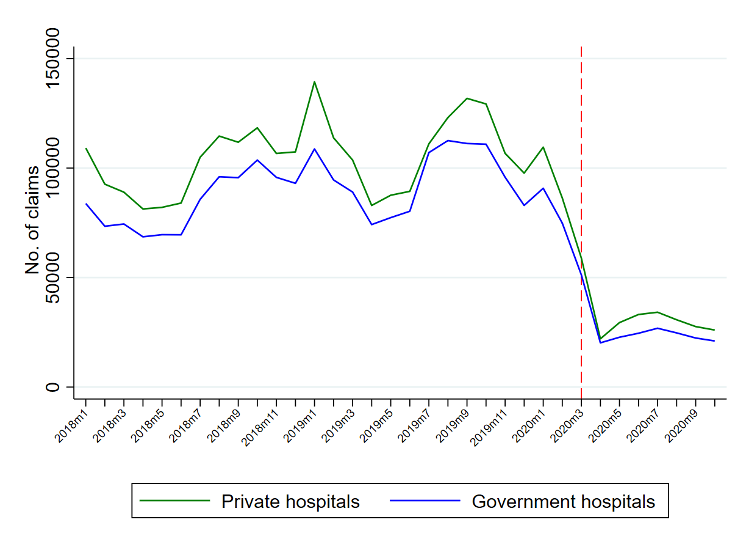
Source: Authors’ analysis of PhilHealth data. Note: the red line indicates the month when the government declared a public health emergency and lockdown (March 2020)
Except dengue fever, the number of claims of the 11 diseases examined in the study have declined precipitously but at varying levels. Alarmingly, the average total monthly claims in 2018 and 2019 have declined more by than 100 percent for diseases such as gastroenteritis, asthma, COPD, diabetes, hypertension, ischemic heart disease, pneumonia, and tuberculosis during the pandemic period. We have not observed significant recovery in the number of claims in the second and third quarters of 2020.
Figure 2. Total claims by high-burden disease, Jan 2018 – Oct 2020
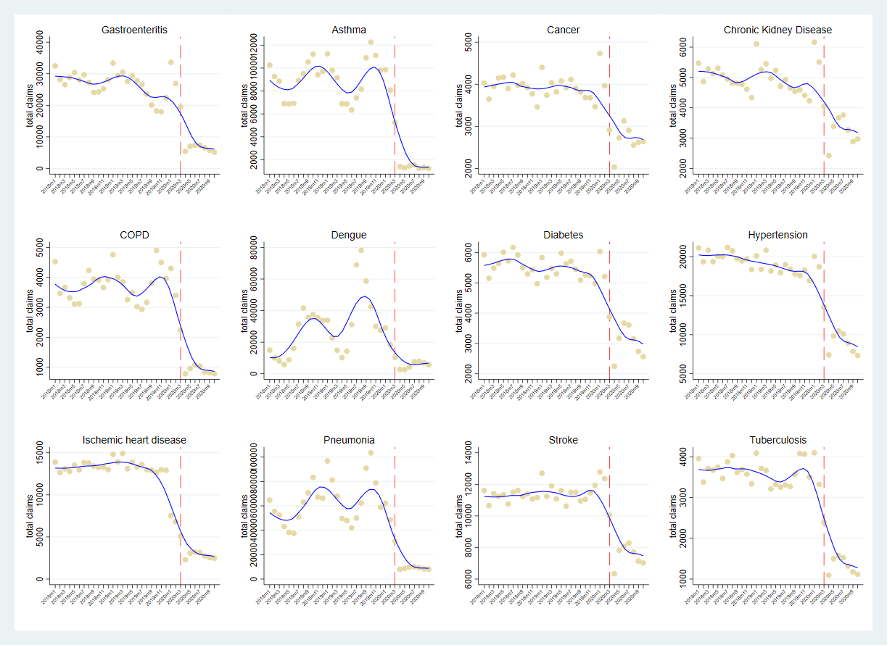
Source: authors’ analysis of PhilHealth data. Note: the red line indicates the month when the government declared a public health emergency and lockdown (March 2020)
How about social health insurance claims for medical procedures? Urgent surgeries or procedures such as chemotherapy should be prioritized over less urgent, elective health care. Figure 3 shows the relatively stable claims for chemotherapy , but a sharp decline for cataract removal surgery. This supports the anecdotal evidence that many hospitals temporarily halted or reduced healthcare services.
There are indications the health insurance claims for child delivery in hospitals have also declined during the pandemic. We need to examine whether there was a shift in preferences to deliver in non-hospital facilities such as maternity clinics or primary care facilities. The government discourages mothers from delivering at home to reduce the risk of infant and maternal deaths, which the country has been relatively successful with in the past decades. There is no compelling evidence yet of increasing home-based deliveries because of the pandemic.
Figure 3. Total claims for chemotherapy, cataract removal, and child delivery, Jan 2018 – Oct 2020

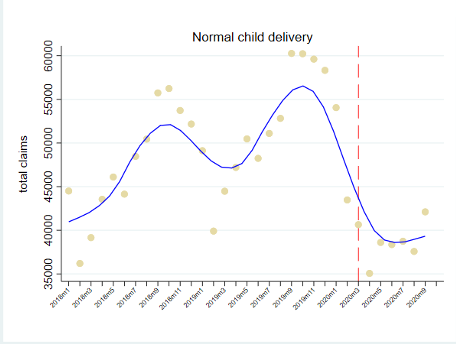
Source: authors’ analysis of PhilHealth data. Note: the red line indicates the month when the government declared a public health emergency and lockdown (March 2020)
COVID-19’s collateral damage
Our preliminary analysis suggests that the COVID-19 pandemic, and the associated policy responses of the government, have led to unprecedented indirect health consequences in the Philippines. The country’s economy declined by almost 10 percent in the past year, one of the largest contractions in the world. This economic tragedy will have enormous effects on people’s income and well-being. However, another immediate and critical consequence, but often overlooked and unmeasured, are the broader impacts of the pandemic on population health, which make the health and economic costs of the pandemic and the associated responses grossly underestimated. Our preliminary analysis of claims data provides strong support for growing concerns about the broad public health impact of the pandemic on non-COVID-19 patients. It warrants a more in-depth analysis of hospital admissions data and mortality data from vital statistics to support our findings. We plan to share a more detailed paper in the coming months.
Topics
DISCLAIMER & PERMISSIONS
CGD's publications reflect the views of the authors, drawing on prior research and experience in their areas of expertise. CGD is a nonpartisan, independent organization and does not take institutional positions. You may use and disseminate CGD's publications under these conditions.
Thumbnail image by: Adobe Stock

