Recommended
In a recent press release, researchers at Oxford University have found that the cheap and widely available drug dexamethasone can be effective in severe forms of COVID-19 in the UK.
Since then, reports have emerged that countries are incurring drug shortages. In fact, the UK has placed export restrictions on dexamethasone and panic buying has started with people buying dexamethasone from local markets or pharmacies in low-resource settings.
Recently, the Africa Centers for Disease Control and Prevention (Africa CDC) also released a statement which provides guidance and recommendations on the use of dexamethasone in severe patients.
Transferring evidence from high-income countries to low-resource settings can sometimes lead to more harm than good. For example, the use of dexamethasone for preterm deliveries in resource limited countries did not decrease mortality in this group and increased in the population overall.
Here, we discuss how transferable the RECOVERY trial dexamethasone findings are to low-resource settings, and derive the following three recommendations when generalising the RECOVERY trial results to low-resource settings:
- Transferring the RECOVERY trial results to lower resource settings, should be done with caution considering the vast differences in population, differing ages, household sizes, comorbidities, and current standards of care.
- Further evidence is needed on the impact of dexamethasone (and other treatments), in severe and critically ill patients who have limited or no access to oxygen or mechanical ventilation.
- Scaling up oxygen availability in LMICs would save lives and increase our confidence in the benefits of dexamethasone.
We strongly conclude that pragmatic trials and early health technology assessments be conducted in different resource-settings and contexts to understand the potential added value of treatments such as dexamethasone.
The RECOVERY Trial
The RECOVERY trial, an open-label, large, pragmatic, adaptive randomised controlled trial in the UK, is currently testing multiple treatments in severe and critical COVID-19 patients. Interim results from the RECOVERY trial find no beneficial effect for hydroxychloroquine or lopinavir-ritonavir in patients hospitalised with COVID-19.
Preprint trial results have shown a positive impact of dexamethasone for severe and critical COVID-19 patients. Dexamethasone reduced 28−day mortality by 35 percent in COVID-19 patients receiving invasive mechanical ventilation and 20 percent in patients receiving oxygen. Dexamethasone also reduced the number of patients progressing from oxygen to invasive mechanical ventilation or death.
When calculating the numbers needed to treat, one additional life would be saved for every 8.5 patients receiving invasive mechanical ventilation with dexamethasone, and the treatment of 25 patients receiving oxygen with dexamethasone would save one further additional life. These are impressive results by clinical standards.
However, dexamethasone did not reduce 28−day mortality in patients who were not receiving respiratory support (Figure 1).
Figure 1. Effect of allocation to dexamethasone on 28−day mortality by level of respiratory support received at randomization
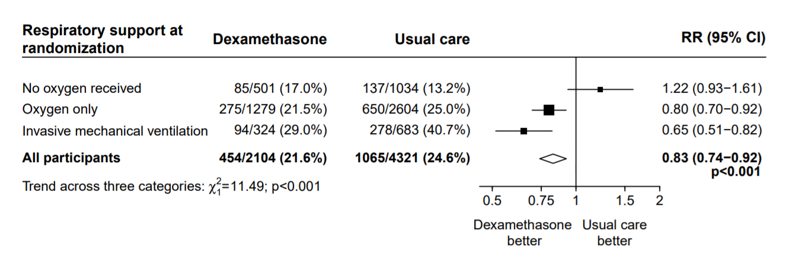
Source: Medrxiv
How similar is the RECOVERY trial population to populations in low-resource settings?
Severe and critical COVID-19 is currently highly concentrated at older ages, particularly those aged 80+. In addition, factors such as comorbidities, household size and contact patterns are all considered to be significant risk factors for severe illness regardless of age.
The mean age of the RECOVERY trial participants in the dexamethasone arm was 66.9 years and in the control arm was 65.8 years. Thirty-six percent of patients were female and approximately 56 percent of the trial population had at least one comorbidity.
It is well known that higher income countries tend to have older populations, household sizes tend to be smaller, and populations have a higher burden of non-communicable diseases (e.g. cancer, diabetes, etc.). In contrast, lower-resource settings have a much smaller proportion of the population who are above 65, with larger household sizes. The population in these countries also tend to have a dual burden of communicable (e.g. HIV/AIDS and TB), non-communicable (e.g. diabetes), and poverty related health issues such as malnutrition. Dexamethasone is an immunosuppressant, and its effect in COVID-19 patients with comorbidities that reduce immunity are not known.
The RECOVERY trial was conducted in the UK and transferability of findings to populations in low-resource settings with differing ages, household sizes, and comorbidities should be done with caution.
Does context matter?
Critically ill patients in high-resource settings are cared for in intensive care units equipped with modern infrastructure and high-tech equipment including mechanical ventilators. In addition, these well-resourced settings are likely to have access to highly trained staff that can deliver advanced critical care.
Within the RECOVERY trial, 2104 patients randomly allocated to receive dexamethasone were compared with 4321 patients concurrently allocated to usual care. Approximately 60 percent of all patients were receiving oxygen at randomization and 15-16 percent of patients were receiving invasive mechanical ventilation.
In comparison, hospitals in low-resourced settings consistently lack capacity to provide oxygen. For example, data from hospital wards in Malawi showed that 89 percent of hypoxic patients (oxygen saturation <90 percent) were not receiving oxygen.
The availability of mechanical ventilation in lower-resource settings is even more sparse. South Sudan, a nation of 11 million, has four ventilators, the Central African Republic has three ventilators for its five million people. In Liberia, which is similar in size, there are six working ventilators. Ten countries in Africa have none at all.
Invasive mechanical ventilation is also an expensive intervention associated with considerable mortality and a high rate of iatrogenic complications in many LMICs. Despite this, much global attention has been directed towards expensive, high-tech equipment that demands highly trained providers while neglecting low-cost essential care.
The usual care provided in the RECOVERY trial involved high-tech modern equipment and well-trained staff. In comparison, in low-resource contexts, equipment, infrastructure, and trained staff to provide critical care, are limited. The hugely different contexts are likely to affect the benefits of dexamethasone.
Can the RECOVERY trial results be applied to a low-resource healthcare setting?
Although the dexamethasone findings in RECOVERY look promising for high-income settings, the benefits for patients cared for in low-resource healthcare settings is less clear.
Based on preliminary trial results and expert clinical opinion, the following matrix highlights the strength of evidence the RECOVERY trial has generated for using dexamethasone in differing COVID-19 severity stages (Figure 2).
Figure 2. Evidence matrix - Mapping the evidence from the RECOVERY trial for dexamethasone in mild/moderate, severe, or critical patients in settings with different availability of resources for respiratory support
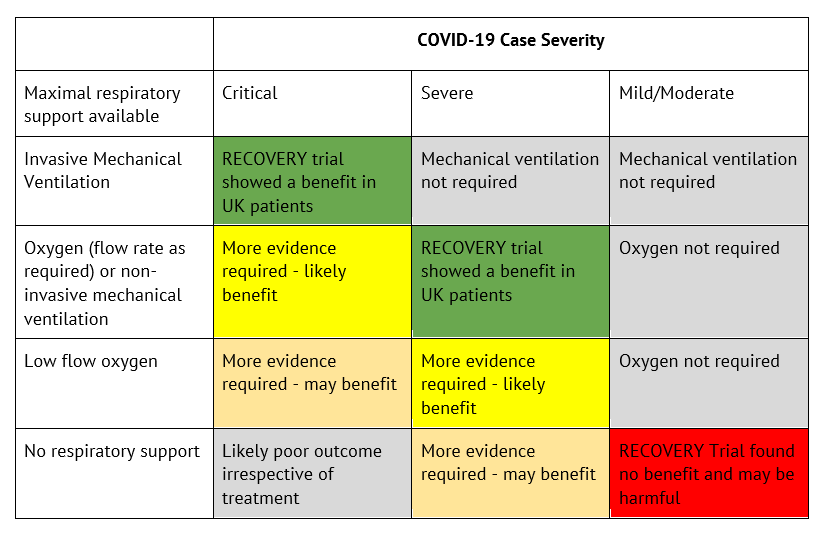
Note, this figure assumes the same population characteristics and patterns of comorbidities as in the UK cohort.
Context-specific evidence is needed on the impact of dexamethasone (and other treatments), in severe and critically ill patients who have limited or no access to oxygen or mechanical ventilation.
Modelling the impact that dexamethasone could have had on COVID-19 deaths in India
As of July 2, 16,475 people have died due to COVID-19 in India. Within this low-resource context, COVID-19 transmission is currently concentrated in densely populated cities, with media reports suggesting 80 percent of cases are in urban areas. However, recently, rural parts of India have also begun to see a surge in infections.
Indian clinicians have suggested that in urban areas, 90-95 percent of patients who died of COVID-19 had received oxygen therapy, and approximately 2 percent of patients who died of COVID-19 had received mechanical ventilation.
In rural areas, oxygen availability has been a greater challenge, with clinicians suggesting that 40 percent of patients who died from COVID-19 had received oxygen therapy, and only 0.5 percent of patients who died from COVID-19 had received mechanical ventilation.
Using this information, we crudely estimate the potential deaths that may have been averted if dexamethasone had been administered as per the RECOVERY trial protocol in an Indian setting (Figure 3).
Figure 3. The potential impact of dexamethasone if it had been given to the patients who died in India as per the RECOVERY Trial protocol
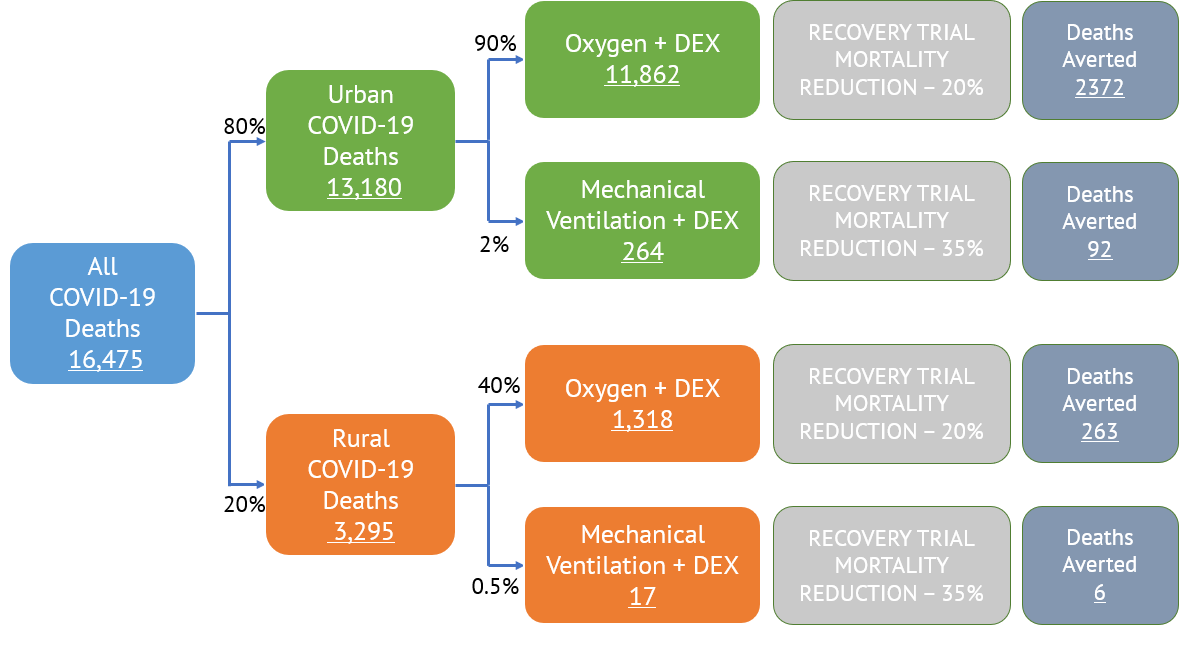
Note: We assume that 80 percent of the deaths occurred in urban areas and 20% occurred in rural areas. Based on anecdotal evidence stated above, we assume conservative parameters of the percentage of deaths that would have either been on oxygen with non-invasive mechanical ventilation or on invasive mechanical ventilation within each rural or urban context and multiply these estimates by the 28-day mortality reduction found in RECOVERY. We make the assumption that all deaths in those who did not receive oxygen or mechanical ventilation were not preventable by dexamethasone.
We estimate that, if the RECOVERY trial results are transferable to the Indian context, approximately 2,733 (16.59 percent) of all COVID-19 deaths in India so far could have been averted if dexamethasone was used as per the trial protocol in patients receiving oxygen or mechanical ventilation. 96 percent of the deaths averted would have been in those receiving oxygen, and 4 percent of the deaths in those receiving mechanical ventilation. An increase in the availability of oxygen in rural areas could have resulted in a great number of deaths averted.
Scaling up oxygen availability in low-resource contexts would save lives and increase our confidence in the benefits of dexamethasone.
Conclusion
The RECOVERY trial results for dexamethasone are impressive and, given it is relatively inexpensive to purchase, governments should be excited by the promise it has shown in severe and critically ill COVID-19 patients in the UK.
In light of these results, governments, multilaterals, and non-governmental organisations will likely already have entered dialogue on pricing and purchasing bulk quantities. However, in low-resource settings, or in contexts where the patient population or health services are different from the UK, evidence to support policy decisions is lacking.
Pragmatic trials and early health technology assessments now need to be conducted in different resource-settings and contexts to test the effectiveness and cost effectiveness of dexamethasone and to help payers (global and national) and technology sponsors understand the potential added value of these treatments when compared to current standards of care.
Disclaimer
CGD blog posts reflect the views of the authors, drawing on prior research and experience in their areas of expertise. CGD is a nonpartisan, independent organization and does not take institutional positions.



