In 2020, epidemiological modelling went from relative obscurity to being central in helping governments, and the public, understand COVID-19 as it spread around the world. In 2021, with the emergence of effective COVID-19 vaccines, Health Technology Assessment (HTA) will be critical to making the best possible decisions in bringing the pandemic under control, particularly in low-and middle-income countries (LMICs). In this blog we look at the potential of HTA to inform how much vaccine countries should buy, who should pay, and how vaccines can be most effectively delivered. We highlight the need for country-level HTA committees, supported by strong regional actors; note the importance of understanding and distinguishing between global health security benefits and local benefits; and unpack how non-standard HTA elements such as macroeconomic and supply chain analysis will be key to COVID-19 decision making on vaccine delivery. Ultimately, if no systematic consideration of the evidence is available, important decisions will be made anyway, potentially misallocating substantial resources and undermining the pandemic response.
The need for HTA to inform COVID-19 vaccine procurement and delivery
COVID-19 continues to be a global public health and economic emergency; over two million people have died, there are an estimated 140 million additional people living in extreme poverty and, in many LMICs, cases are once again on the rise. A range of effective vaccines are now becoming available (summarised in Table 1) and calls to ensure their availability in LMICs have gone beyond well beyond public health audiences to mainstream media. There is a clear need to support LMICs but there are some difficult questions too. Should everyone who wants a COVID-19 vaccine get one? Are some vaccines worth more? And given local epidemiology and ability to pay, who should finance the vaccine and in what share? And what if, in some contexts, there are better uses of the money?
COVAX, the initiative to support COVID-19 vaccination in LMICs involving WHO, Gavi, CEPI, and UNICEF, has committed to provide sufficient doses for at least 20 percent coverage in participating countries. While the potential efficacy of vaccines against transmission (rather than clinical outcomes) will begin to emerge over the coming weeks, the coverage required to bring the reproductive number below one in absence of physical distancing measures will differ between countries and is very likely to be greater than 20 percent. Africa CDC is currently working with member states of the African Union towards a goal of 60 percent coverage and estimate it could cost as much as $7-10 billion for the vaccine and the systems and structures required for delivery. On a continent where per capita annual health expenditure can be as little as $30, care should be taken to be sure resources are used in the best way. For example, Uganda recently ordered 18 million doses of the Oxford AstraZeneca vaccine, on top of 3.5 million to be provided by COVAX. This purchase is expected to cost $17 per two dose course, including handling and transportation, a substantial amount considering the total per person health spend in 2018 was just $43.14.
Defined by WHO as “the systematic evaluation of properties, effects, and/or impacts of health technology,” Health Technology Assessment, a process involving economic evaluation, key stakeholder input and an explicit consideration of trade-offs, offers a framework to help address these questions. Economic evaluation (cost-effectiveness and related analyses) is typically a key part of HTA but importantly the approach can bring together a range of different types of quantitative and qualitative evidence (such as equity and budget impact) into a single decision-making process. The World Health Assembly had previously urged member states to use HTA as a key tool to help define benefits as part of universal health coverage efforts.
Building on an earlier CGD Blog, we outline two applications of HTA to inform decisions on COVID-19 vaccines, both of which are important in the near-term initial vaccine roll-out but will remain relevant as COVID-19 likely becomes an endemic disease.
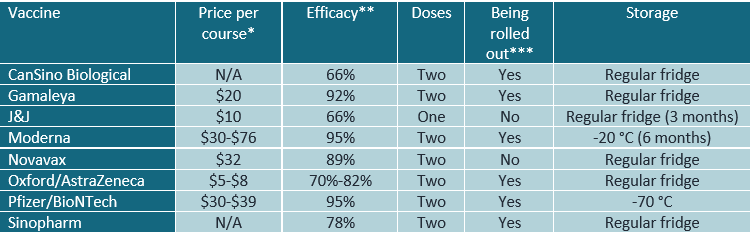
Table 1. Summary of a subset of COVID-19 vaccines that have published phase III trial results
* Prices vary by country based on the deals negotiated and in some cases there was a lump sum payment which have reduced the per vaccine price, and much of this information is not public. Here we compiled public information on the price for a full course of each vaccine, Information is from the Washington Post, Sky News and the Wall St Journal.
**Efficacy is reduction in disease from the original variant.
*** Being rolled out anywhere as of the 16th of February 2021 according to LSHTM.
1. How much should countries be prepared to spend on COVID-19 vaccines?
To address this, HTA considers the full costs and consequences of vaccination, which, for regular vaccination services broadly includes:
- Vaccine purchase cost;
- Vaccine delivery;
- Health protection to individuals vaccinated;
- Indirect protection to the wider population and;
- The reduced cost of illness resulting from direct and indirect protection.
Over the past decade, dynamic infectious disease models have increasingly been used to assess the full effects of vaccine interventions and examples of this kind of economic evaluation for COVID-19 response are being done, see c19economics.org for more. It will also be important to account for any effects of COVID-19 vaccination on displacing or, in some cases allowing the resumption of, other essential health services.
However, COVID-19 is radically unlike other vaccine preventable diseases in the degree to which the spread of the disease requires lockdown-like public health measures or other interventions that dramatically affect whole economies and livelihoods. While it has not previously been standard practice, HTA of COVID-19 vaccines must also consider macroeconomic effects, or risk missing an important part of the picture (see this example from the US or this one from the UK) (recognising that other major disease control initiatives may also have some macroeconomic effects). Moreover, COVID-19 has highlighted that we live in a globally connected world and uncontrolled transmission in one country leads to the exportation of cases, and even knock-on economic effects, to other countries. In other words, more than any previous disease, global health security is a major factor in motivating COVID-19 control.
Figure 1. Summary of costs and consequences to consider in COVID-19 vaccine HTA

For a complex public health problem like COVID-19, “value for money” will mean different things to different people and, as always, decision-making comes down to opportunity cost and perspective. For many LMICs, the very significant pre-COVID health challenges will mean that, at a certain point, additional spending on COVID-19 vaccination is no longer good value in terms of health gain compared to alternative ways to spend on health (increasing coverage of basic primary healthcare for example). Therefore, from a national perspective only, countries might reasonably choose lower coverage or a cheaper, less efficacious vaccine with lower impact on COVID-19 transmission. However, the externality risk to the rest of the world, including the risk of “vaccine insensitive” variants arising in situations of uncontrolled spread, highlights an “enlightened self-interest” reason for high-income countries to support COVID-19 vaccination in poorer countries given the risk to their societies and economies at home. This in addition to compelling cases to be made on the basis of ethics or equity. Indeed, high-income countries and multilateral institutions must avoid pressuring LMICs to spend their own scarce resources on COVID-19 vaccines if it means diverting spending from other uses that would yield greater benefits in those countries. In other words, the global community must recognise when the principal justification for COVID-19 control via immunisation is global health security, rather than health benefit in a low-income country where populations are young and other health problems more significant.
It will not be possible (or desirable) to quantitatively aggregate all relevant evidence on these complex and wide-ranging factors in an economic evaluation. Equally, good quality data will not be available for many key factors. Nevertheless, HTA can support a structured and deliberative process, taking into account practical constraints such as which vaccines are available to procure and have suitable cold chain requirements, to enable decision makers to consider the various aspects of this complex but essential question and identify priorities for gathering more information.
2. Designing delivery: What HTA can offer vaccine campaign planners
COVID-19 vaccine procurement is just the beginning. The HTA process can also support the prioritisation and planning of a cost-effective approach to the delivery of COVID-19 vaccination. Currently there are significant global concerns on whether suppliers can meet the increasing need for a vaccine in countries that are having to deal with new variants and a second wave. Further uncertainties also lie in the national distribution of these vaccines to remote and rural areas such as issues in supply chains (e.g. lack of a cold chain) or in countries where the private or not-for-profit sector represent the bulk of healthcare utilisation. Variability also exists across countries in trying to understand which populations should be prioritised for vaccination (e.g. vaccinating elderly versus working population, or a geographic or hot spot strategy rather than demographic group approach) is the most effective at controlling the epidemic within the limited resources available.
Given the large uncertainties in global manufacturing and distribution alongside the uncertainty involved in vaccine impact and characteristics, quantifying and identifying optimal vaccination strategies through a formal Health Technology Assessment is needed. Appraising such evidence in a larger HTA process that accommodates deliberation and value judgements, can aid decision makers in implementing large scale mass COVID-19 vaccination programmes that account for epidemiological, economic, clinical and supply chain constraints, and other limitations.
Health Technology Assessment, supported by well-established economic evaluation methods, can aid in calculating the number of vaccines needed over time, assess whether a country has significant capacity to meet demand, quantify the potential costs involved with differing vaccines and vaccine implementation, identify potential bottlenecks in supply chains that may lead to inefficiency and identify the most cost-effective and optimal strategy from a healthcare and societal perspective that will control COVID-19 both nationally and globally.
Recommendations
Health Technology Assessment can help countries and international donors make critical decisions about COVID-19 vaccines, both in the near-term, and as COVID-19 becomes an endemic disease. Ultimately, if no systematic consideration of the evidence is available, important decisions will be made anyway, potentially misallocating substantial resources and undermining the pandemic response.
Countries need to set up rapid and light touch COVID-19 vaccine HTA committees to gather and review the available evidence, likely in partnership with National Immunisation Technical Advisory Groups.
However, it is neither efficient nor realistic to expect full in-depth technical analyses to be conducted in all countries. Regional bodies can provide support by i) conducting or coordinating regional multi-country analysis ii) providing Covid-specific and context relevant HTA guidance and iii) facilitating model and evidence sharing between countries and regions. The International Decision Support Initiative, an initiative in which CGD participates and serves as secretariat, is working in partnership with Africa CDC to support HTA in the region, starting with case studies in Nigeria, Ethiopia, and Kenya.
COVID-19 HTA will be different from business-as-usual HTAs. The enormous whole-of-society effects mean the scope of the assessment cannot be limited to the health sector. Moreover, quality data will be scarce in many key areas, particularly at first. Initial HTAs must help identify the priority areas for further research.
Vaccine coverage decisions based on country-level HTA may under value a socially optimal level of vaccine coverage from a global perspective. Multilateral organisations, including WHO and the World Bank, must work with countries to understand and communicate the value of global health security and therefore “enlightened self-interest” such that this global public good is financed collectively in low-income countries.
Disclaimer
CGD blog posts reflect the views of the authors, drawing on prior research and experience in their areas of expertise. CGD is a nonpartisan, independent organization and does not take institutional positions.




{kind=link}