Recommended

India’s COVID-19 crisis is tragic but not unprecedent or unexpected.
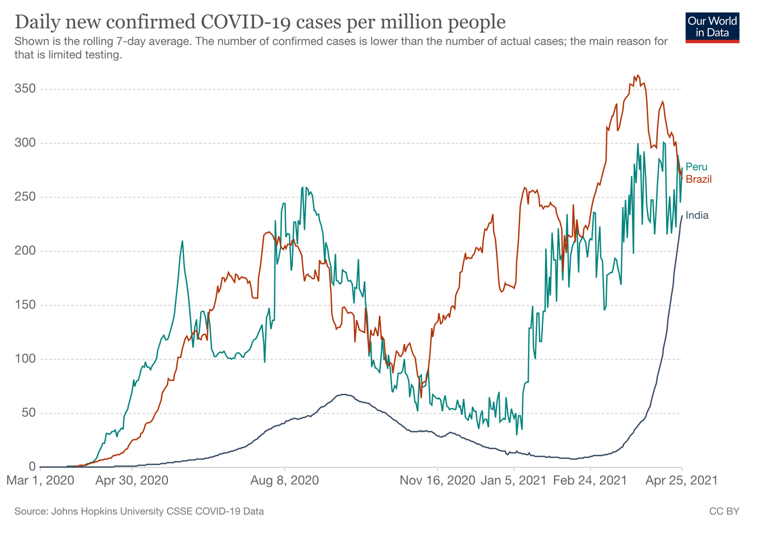
India’s second COVID-19 wave has been explosive, reaching world record totals of over 300,000 daily officially reported cases. The true number is likely to be much higher, with a large number of cases missed as indicated by the delays in testing and rapidly rising positivity rates - currently one in every four people tested are positive for COVID-19 across India. Leading models estimate that there could be over 1 million cases per day. The health service has collapsed, with queues of ambulances parked outside full hospitals, oxygen and drug shortages in multiple states, and life-saving non-COVID services interrupted.
On April 26th, India reported 2,480 COVID-19 deaths; this will certainly rise over the next few weeks, with case numbers showing no sign of abating. The true estimate is likely to already be higher than this – as non-stop cremations cast doubt on India’s counting of deaths. Some districts are reporting COVID-19 deaths several times less than COVID-19 cremations and this disparity is raising further questions about the quality of the data collected. With the considerable concerns about both case counts and mortality data, the risk is that the Indian government is “flying blind,” unable to identify hot spots, plan services, and optimally guide the response.
This situation is not unique to India. It has happened (and is still happening) across South America, as of this week countries such as Brazil and Peru are suffering higher per capita cases than India. Notably, the United Kingdom reported a four times higher infection rate per person back in January of this year. This situation was also not fully unexpected, as modelling groups had predicted early in 2020 that very large outbreaks in LMICS were likely. The tragedy in India is not the existence of the second wave, but the fact that India did not learn from the experience of Brazil, Peru, the UK, nor even the first Indian wave, and did not prepare adequately when it had the chance. For example, healthcare facilities set up in preparation for the first COVID-19 wave were prematurely closed down earlier this year.
In this blog, we look at three urgent actions that India (including its state governments) can take now to mitigate the disaster. It is a very challenging situation, as nationwide lockdowns are unlikely to be sustainable and effective in India’s economic context. Most of the actions are also politically costly in the short term (e.g., requesting international support), but will reap political benefits in the long run if they help bring the pandemic under control. This is not business as usual, but a deep and deadly crisis, and the government must take decisive action. Unfortunately, at this stage of advanced exponential growth, it is likely that all three action areas will not be enough to bring R under 1 by themselves. Cases will therefore continue to rise and total mortality can be expected to be high.
Perhaps the most important lesson is for other countries, and the international community, to now learn from India and prepare better for the next wave.
Action 1) Focus the health service on scalable and essential lifesaving COVID-19 treatments and protect other life-saving essential services.
In the short term the health service will need to pivot towards providing efficient COVID-19 care, whilst maintaining only the most essential routine services. This means focusing on basic approaches that saves lives and are scalable – such as essential emergency and critical care (EECC), oxygen, triage and dexamethasone. The Ministry of Health in India has appropriately updated clinical treatment protocol and restricted the use of therapeutics with limited or no clinical effectiveness evidence such as Remdesivir, Convalescent Plasma and Tocilizumab. Advanced therapies such as mechanical ventilators that are difficult to scale up for a crisis of this magnitude should be a lower priority.
Rapidly scaling up oxygen capacity is the priority of the hour. Several Indian cities have issued an SOS stating that hospitals are left with only a few hours of oxygen supply. There are widespread reports of patients dying with oxygen running out. India is currently reported to be dipping in to its oxygen reserves. The Government has already diverted all industrial oxygen for medical use and issued a tender to import 50,000 MT of liquid oxygen.
India now needs to urgently increase in-country oxygen production, import additional oxygen, and address the adequate and safe transport of oxygen via train, road, and air over large geographical areas since not all states manufacture oxygen. States such as Kerala that have a surplus of oxygen have already been supplying to other states; however, it is necessary for there to be improved dialogue between states and larger scale coordination across the entire country in order to move oxygen supplies to where they are needed most, minimising issues such as hoarding.
Finally, many essential and lifesaving services for non-COVID-19 illnesses will be interrupted, resulting in additional loss of life. Health service planners will explicitly need to consider the impact of focusing on COVID-19 as opposed to other essential health services. It is important for guidance to be published on the services that are essential and ensuring that these are protected whilst others are paused.
Action 2) Expand and maximise health service capacity by bringing in the military, leveraging home-based care, and mobilizing international support.
Given that the current wave of infections in India has overwhelmed the healthcare system, there is a dire need to increase healthcare capacity. This will be challenging considering the time frame required to scale up resources and personnel. However, the longer these decisions are delayed, the greater the mortality impact. Here we outline key recommendations that can be taken to increase health service capacity.
First, military resources and central government resources should immediately be used to assist the civilian response to the COVID-19 crisis. This has already begun with the Indian military providing oxygen from armed forces reserves, setting up field hospitals, sharing transport services (e.g., military ambulances, interstate and international oxygen airlifts) and opening up existing military medical infrastructure to civilians. However, the Indian military can also provide additional services and resources such as non-medical assistance which can include logistics, planning, and storage and packaging of personal protective equipment. Given that India has the world's second-largest military force and has the world's largest volunteer army, such additional personnel and resources can be pivotal in aiding the COVID-19 response.
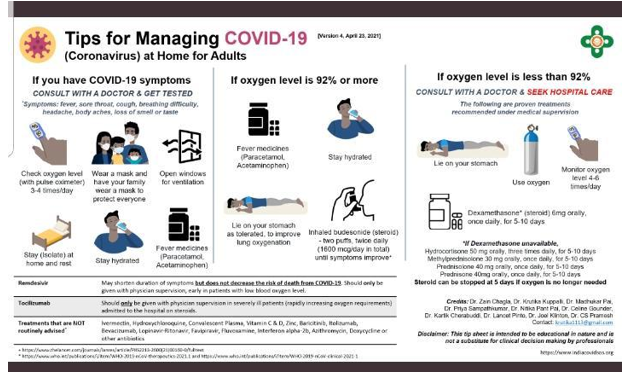
Secondly, to ease the intense pressure on beds, medical research bodies should be releasing and promoting citizen friendly guidelines for when patient can be safely treated at home to save spaces for more severe patients. For example, Figure 1 shows evidence-based guidance and tips for home-based care developed by clinicians which is available in six Indian languages. Promoting the use of home-based care, telemedicine, m-health and e-health to control COVID-19 are effective measures that increase the number of patients that doctors are able to see and will expand healthcare capacity.
India can also harness the existing social structures of collective families and volunteers who can provide safe care at home and also contribute to delivery of care in hospitals. This has worked well in some states during the previous wave to both decrease the burden on healthcare providers and provide reassurance to both patients and family members. This further ensures that families remain isolated at home thereby reducing transmission.
Figure 2 shows an infographic developed by Indian clinicians highlighting “Tips for Managing COVID-19" which is available in 6 Indian languages found at https://www.indiacovidsos.org/home-care
Finally, the current epidemic in India is now reaching the level of a humanitarian crisis. Here, the government of India should be focussing its efforts on coordinating an international humanitarian response to improve health system capacity through expanding cooperation with NGOs already present in the country, accepting international cooperation and humanitarian support, and utilising India’s access to IMF and World Bank funds. This has recently begun, with the European Union , the UK, and the US sending oxygen, ventilators and medicines, but more international support is urgently required. The US has now lifted its export ban on vaccine materials which is a welcome, if belated, decision.
Action 3) Strengthen the public health response with short local lock downs, support to livelihoods, clearer communication, and sustainable COVID-19 control measures.
Whilst focusing and expanding the health service will save lives, the biggest impact will come from public health measures. The first measure is to keep the focus of vaccination efforts on those aged 45 and older and health care workers, and not to expand to the over 18s as is planned from May. This will save the most lives in the short term and keep the health service running without overwhelming it. The government must also explore options for making COVID-19 vaccination safer, including by relocating vaccine centres outdoors.
Currently some cities are in a 7-day lockdown. In addition, states in India are now urged to go for an intensive, local, and focused lockdown based on guidance from the Union Home Ministry. The lockdown will be beneficial in buying time to carry out actions 1 and 2: for example fixing oxygen transport challenges and expanding safe vaccine access and administration to the most vulnerable. However, India needs to proactively mitigate the public disorder, mass migration, and panic that a lockdown can trigger (e.g., Delhi).
National or state-level lockdowns will also only be beneficial if livelihoods are protected through direct cash transfers, food provision, and improved public messaging by the Government. This is necessary to make staying at home a feasible option. Here, the international community needs to support India in controlling COVID-19 and could provide loans to support such measures.
This should be followed by a range of sustainable COVID-19 control measures, which may include:
- A focus on moderate but sustainable physical distancing measures: (e.g., prevention of mass gatherings, pausing political rallies, stopping religious festival gatherings, curfews)
- A radical shift and reset in public communication and education campaigns, with leaders modelling behaviours that will decrease virus transmission, supported by community leaders and the mobilization of social media
- Better data collection, including of cases, deaths, and hospital and oxygen capacity monitoring.
Conclusion
India can save lives by focusing the health service on essential COVID-19 and non-COVID-19 care, whilst maintaining a focus on safe vaccine campaigns for people over age 45 and health care workers. India will benefit from recruiting additional capacity by harnessing home-based care, the military, and international partners. Lockdowns will have to be local and brief, and supplemented with livelihood support and a communication strategy reset.
The India COVID-19 crisis is not unexpected and is not without precedent. India could have learnt lessons from the unfolding of the epidemic in Peru, Brazil, and the UK and been better prepared. Now the world needs ensure that the COVID-19 crisis in India ends soon and is not repeated elsewhere.
Disclaimer
CGD blog posts reflect the views of the authors, drawing on prior research and experience in their areas of expertise. CGD is a nonpartisan, independent organization and does not take institutional positions.



{kind=link}
{kind=link}